Flu Shot Verification Form
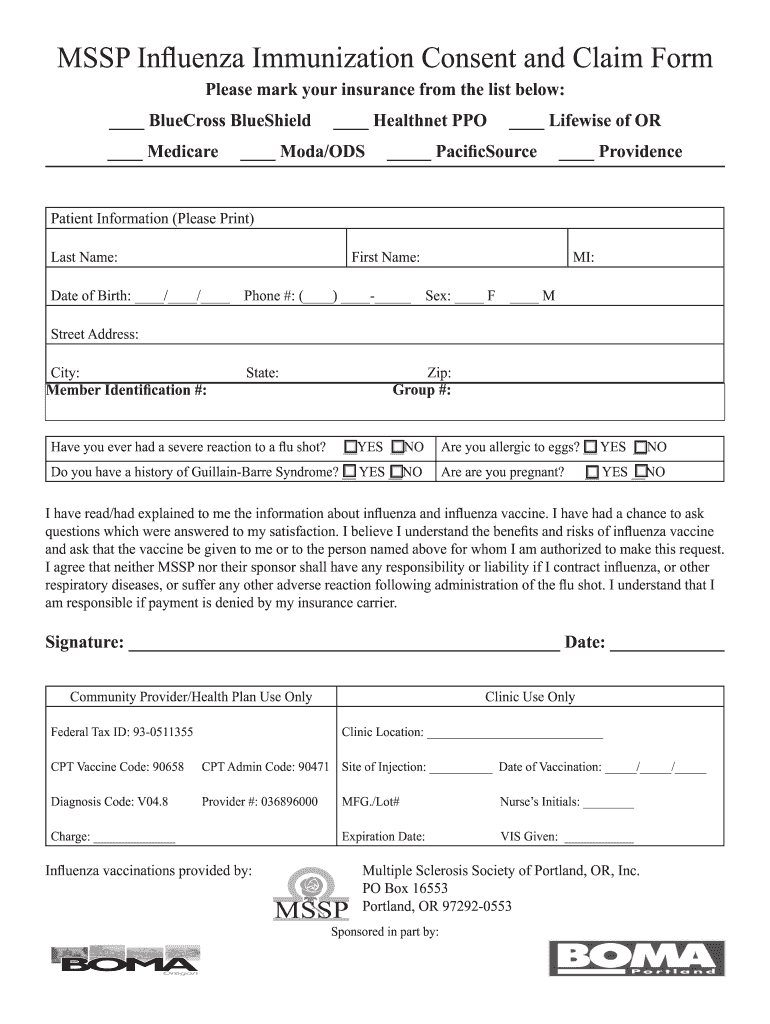
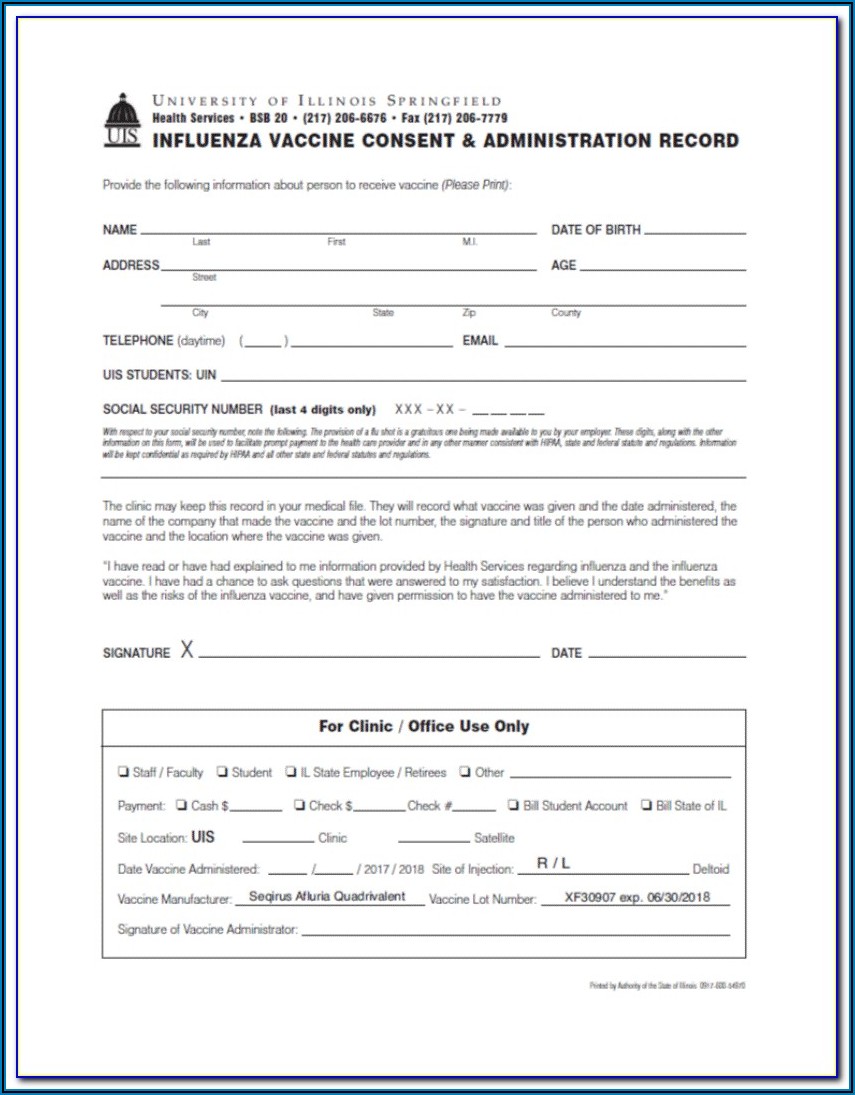
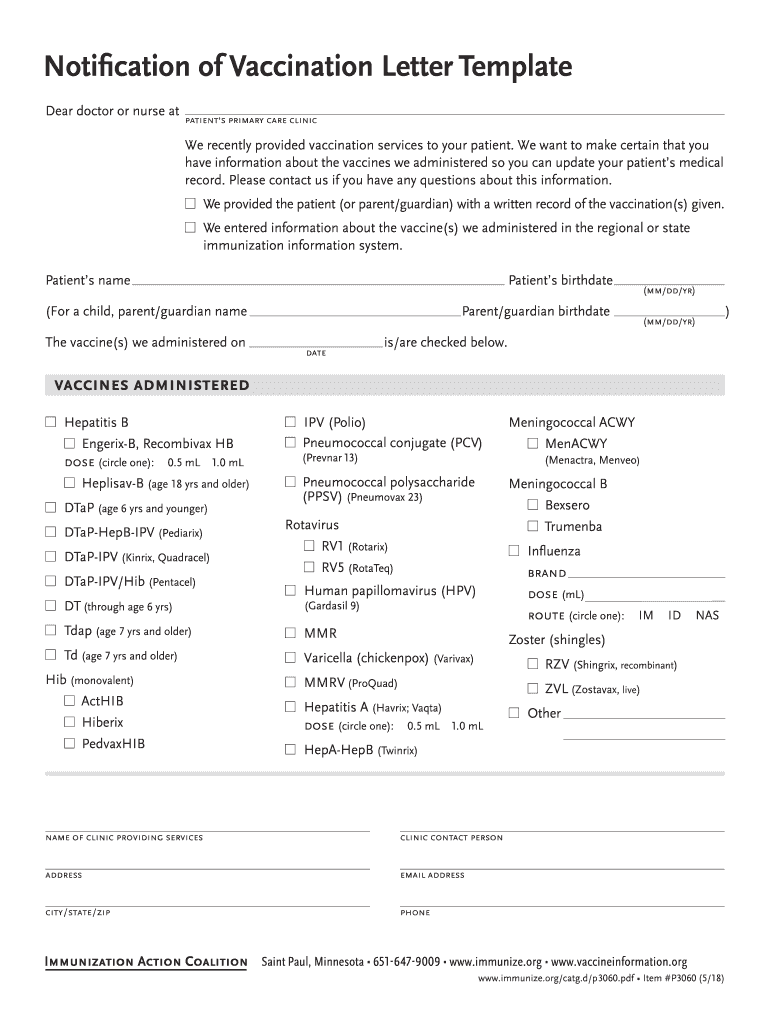
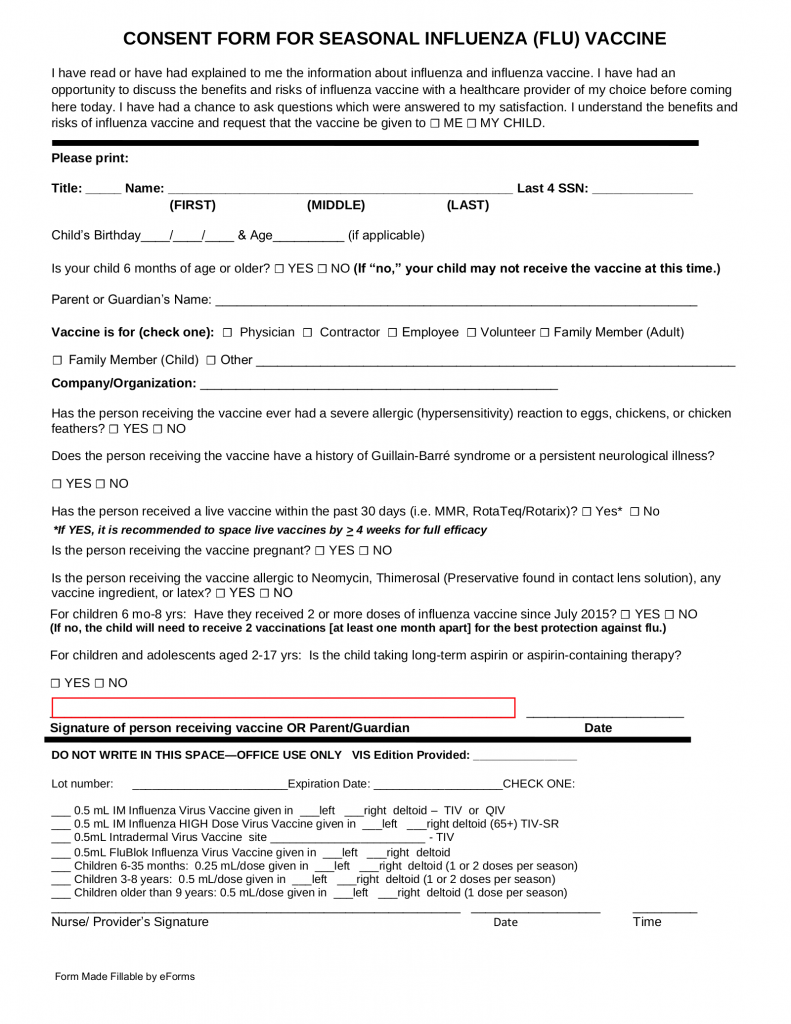
Flu Shot Verification Form - Seasonal influenza vaccination program for vha healthcare personnel. Flu shot verification form name of employee: Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. I have read and fully understand the information on this form. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination.
I have read and fully understand the information on this form. Seasonal influenza vaccination program for vha healthcare personnel. Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Flu shot verification form name of employee:
Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form. Flu shot verification form name of employee: _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below.
Printable Flu Shot Verification Form Printable Word Searches
Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Flu shot verification form name of employee: Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below.
Flu Shot Verification Form Form Resume Examples yKVBbNLoVM
I have read and fully understand the information on this form. Seasonal influenza vaccination program for vha healthcare personnel. Flu shot verification form name of employee: _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below.
Vaccine Consent Form Template
_____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form. Flu shot verification form name of employee: Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below.
Cdc Flu VACcine Consent Form 2019 2020 Printable Consent Form
Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Flu shot verification form name of employee: Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form.
Faceing Math Template Complete with ease airSlate SignNow
Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form. Flu shot verification form name of employee:

Cvs Printable Proof Of Flu Shot Form Printable Word Searches
I have read and fully understand the information on this form. Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. Seasonal influenza vaccination program for vha healthcare personnel. Flu shot verification form name of employee: _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination.

Printable Flu Shot Verification Form Printable Word Searches
Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. Flu shot verification form name of employee: Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination.
Proof of flu vaccine form Fill out & sign online DocHub
_____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Flu shot verification form name of employee: Seasonal influenza vaccination program for vha healthcare personnel. Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. I have read and fully understand the information on this form.

Free Printable Flu Vaccine Consent Form prntbl
_____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Flu shot verification form name of employee: Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. Seasonal influenza vaccination program for vha healthcare personnel. I have read and fully understand the information on this form.
Certified Nursing Assistant Flu Vaccine Verification Qvcc Form
Seasonal influenza vaccination program for vha healthcare personnel. Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. I have read and fully understand the information on this form. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Flu shot verification form name of employee:
I Have Read And Fully Understand The Information On This Form.
Flu shot verification form name of employee: Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. _____ dob:_____ district/college:_____ participant signature:_____ date:_____ vaccination. Seasonal influenza vaccination program for vha healthcare personnel.